
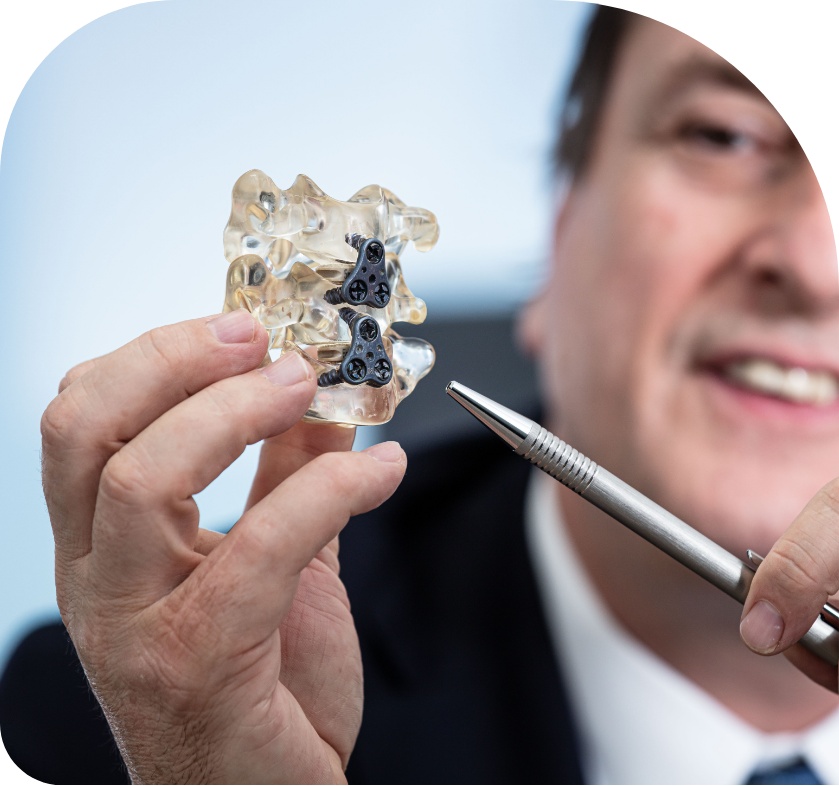
Instrumented spine surgery is surgery performed to treat spinal problems with the use of spinal implants (excluding pain modulation devices).
Instrumented spine surgery can be divided into 2 major categories: Fusion and non-fusion procedures.
Spinal traumatic injuries and degenerative diseases are the most common conditions which might require addition of implants during surgery but a variety of congenital and acquired conditions affecting the spine may also require instrumentation as part of their treatment.
A spine motion segments is defined as two bony levels with an intermediate disc which allows healthy motion to occur. The spinal discs are named after the bones that sit above and below the respective disc. For instance, L4 L5 disc is attached between L4 and L5 vertebral bodies.
Anterior or lateral spinal instrumentation procedure
Anterior spinal instrumentation is usually performed on cervical and lumbar segments, rarely on thoracic level.
At the lumbar segment, anterior approaches to the spine for fusion are becoming increasingly popular as they help restore the correct shape to the spine.
The aim of this surgery is to achieve fusion of the motion segment from an anterior, oblique or even lateral approach by inserting a fusion cage between the vertebral bodies in a minimally invasive fashion.
More often anterior surgery is combined with a posterior approach to achieve optimal fusion. This can be achieved in a single procedure or in a staged fashion.
What to expect following a spinal fusion procedure?
Immediately after your operation, some discomfort can be expected especially at the surgical site.
Every effort will be directed at ensuring the patient’s comfort.
Patient will typically wake up either in intensive care unit or other highly monitored area (post anesthesia recovery area). A staff member will attend to assess the patient’s general health, vital signs, wound dressing and check their neurological function regularly in the initial few hours to ensure the recovery from anesthesia is smooth.
A physical therapist will attend to the patient as soon as advised by the surgeon and the patient will start some physical exercises including walking as tolerated.
Walking early is good for the lungs, circulation and helps prevent the risk of blood clots (Deep Vein Thrombosis- DVT) forming in the legs, hence accelerates recovery.

