What is a Craniotomy?
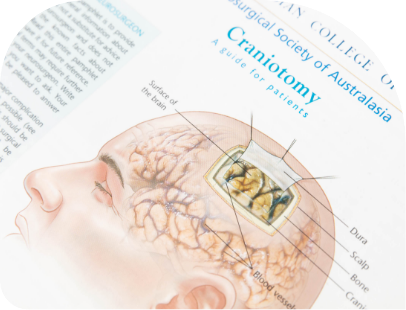
A craniotomy is a surgical procedure aimed to create an opening in the skull (i.e., a bone flap).
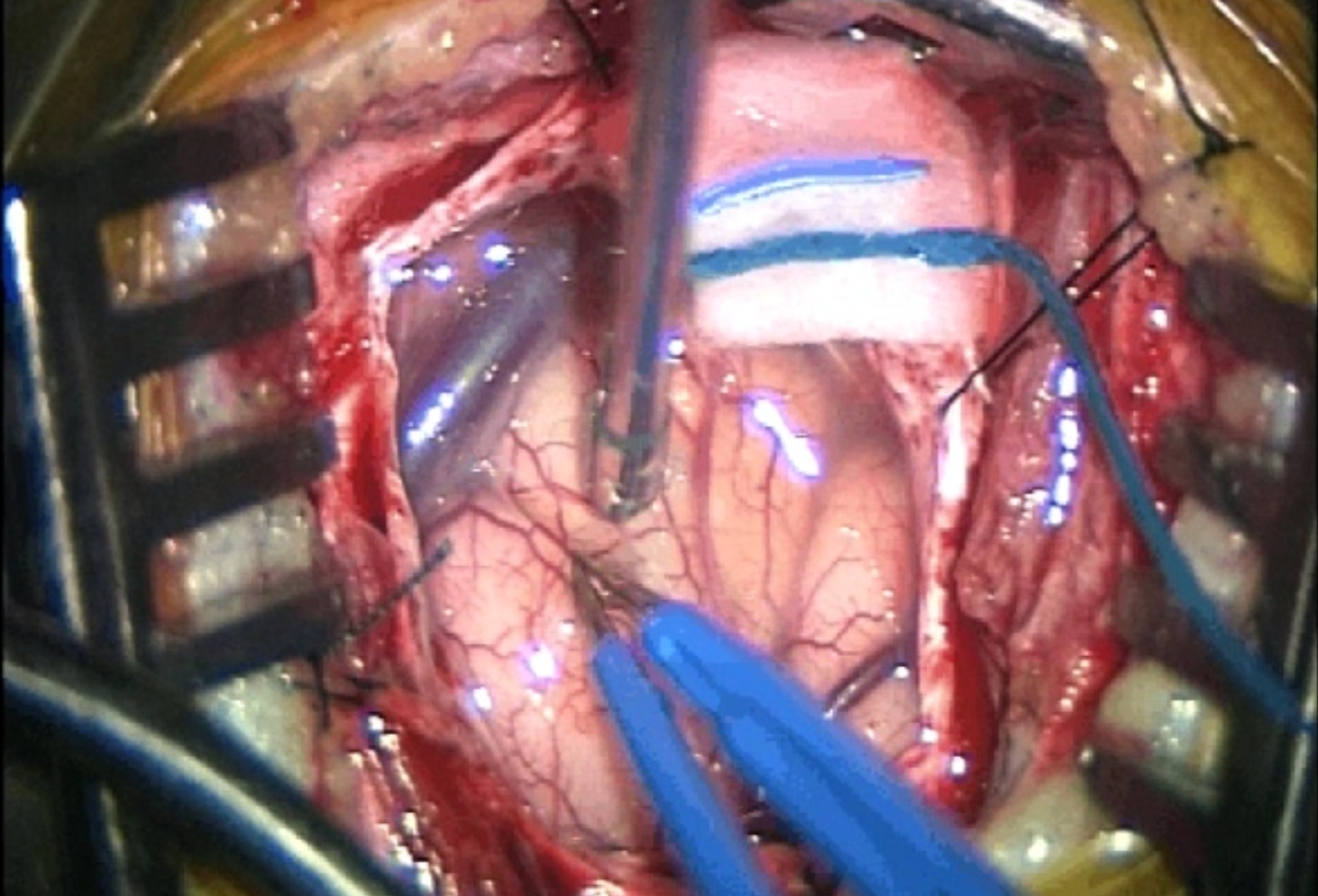
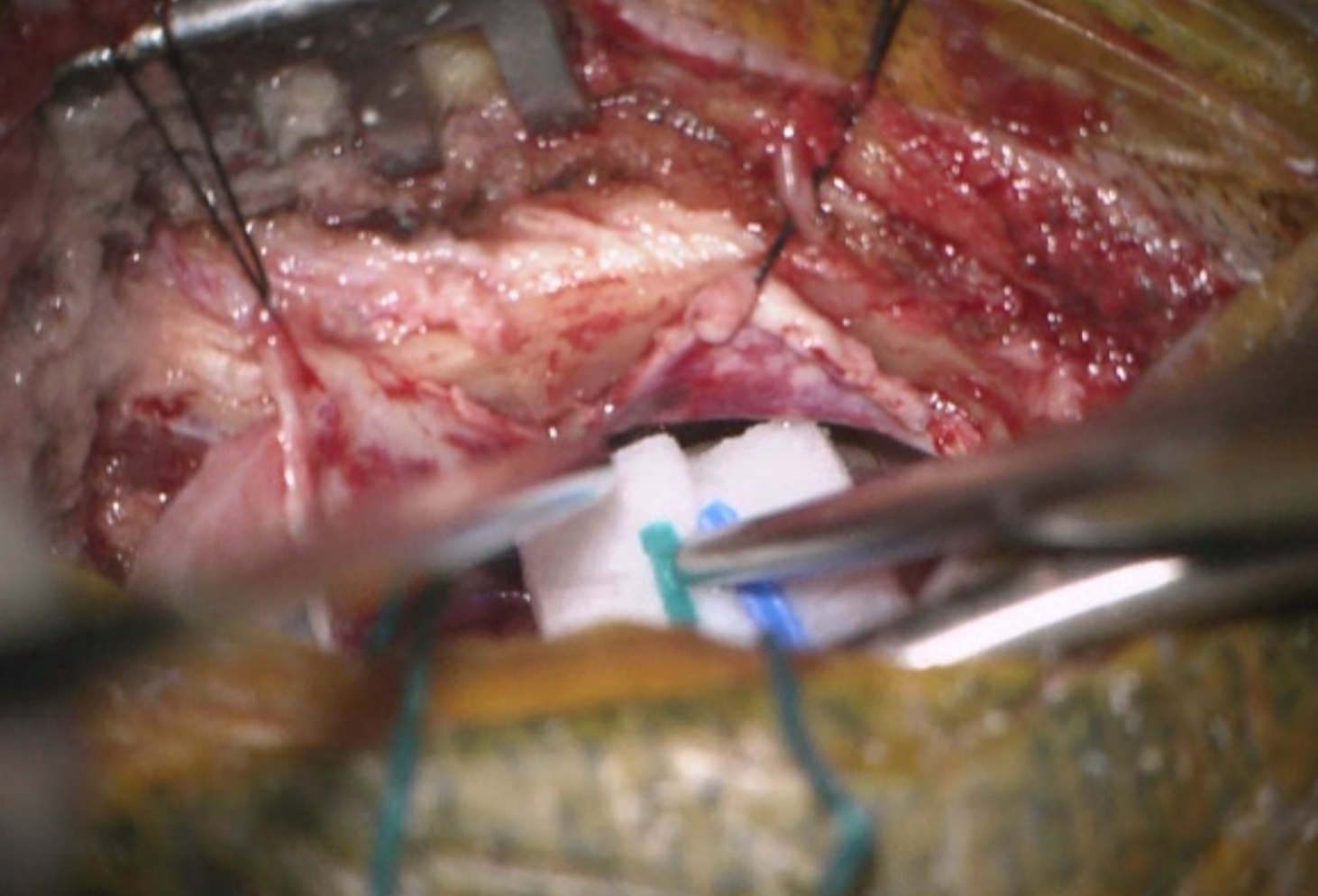
This opening is performed to access the intracranial structures (e.g., the brain underneath) by means of specialised tools. Different types of craniotomies exist, according to the necessity. A craniotomy is performed to treat brain tumours, aneurysms or AVMs, traumatic head injury, hematomas (also called blood clots), infections, or to remove foreign bodies.

Reasons for the procedure
A craniotomy may be done for a variety of reasons, including, but not limited to:
- Performing a biopsy / resection of a brain / skull base tumour
- Clipping or repairing an aneurysm
- Removing blood or blood clots from a leaking blood vessel
- Removing an arteriovenous malformation (AVM) or addressing an arteriovenous fistula (AVF)
- Brain biopsy
- Draining a brain abscess
- Repairing a skull fracture
- Repairing a tear in the membrane lining the brain (dura mater)
- Relieving pressure in the brain after an injury or stroke
- Implanting stimulator devices (for example, for pain treatment or movement disorders such as Parkinson’s disease).

Patients may experience the following:
Nausea, headaches – symptoms that can be controlled by prescribed medications
Swollen and bruised eyes
Head may be elevated to about 30 degrees to reduce the risk of intracranial pressure
They will be frequently asked to move their arms, fingers, toes, and legs
Hospital staff will regularly test for any signs of brain damage – for instance, they may examine the patient’s pupils with a flashlight or ask simple questions
Steroid medication (to control brain swelling) and anticonvulsant medication (to prevent seizures) may be given depending on the type of brain surgery

Until then, follow the surgeon’s care instructions once back home. General suggestions include:
- No heavy lifting
- No strenuous activity including housework and contact sports
- No alcohol drinking, to avoid blood thinning and risk of bleeding, and no alcohol mixing with pain medicines
- No smoking or use of nicotine products such as vape. It may delay healing
- No driving, no flying, no return to work until the surgeon allows
- Gradual increase of the physical activity, starting with 5 to 10 minutes every 3 to 4 hours
- Keeping incision clean and dry: no bath, pool, or tub soaking. No lotion/ointment to be applied, including hair styling products